Drugs of Abuse Urine (DAU)
Lab menu: DAU and oxycodone screen
+Opiates:Indicates any combination of codeine, MSo4, hydrocodone, hydromorphone, oxycodone.
- When ordering DAU, add screen for oxycodone, buprenorphine, and fentanyl.
- Tramadol will not be detected by DAU opiate screen; confirmation required.
DAU tests specifically for cocaine and methadone metabolites benzoylecgonine and EDDP, respectively.
- Nucynta may produce false positive for methadone.
Detection Period
- Opiates: 1-2 days for most, 2-3 days for fentanyl
- Methadone: 3-11 days
- THC: 3 days single use, 4 days moderate use, 10 days heavy use, 30-36 days for chronic, heavy use
- Alcohol: 7-12 hours
- Collection: 50 ml, ward collect.
- Temperature: 90-100 degrees within four minutes of voiding.
- Tampering/Dilution: Order creatinine and specific gravity.
- Urine Creatinine: < 20mg/dl considered dilute.
- Urine specific gravity (SG): 1.002-1.020, SG H20 = 1.0.
- Substitution: pH extremely low < 3 or high > 11.
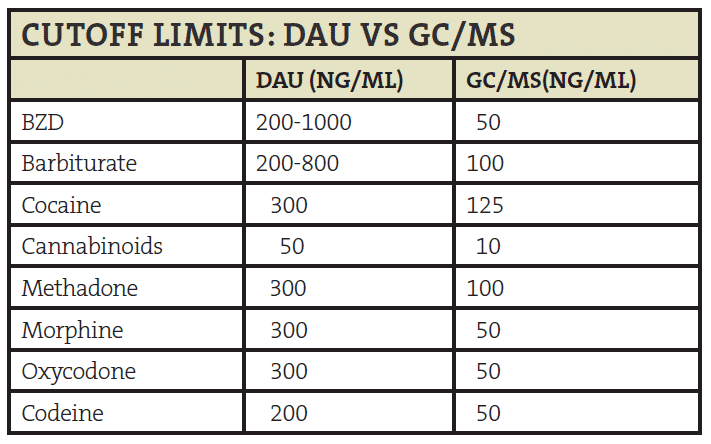
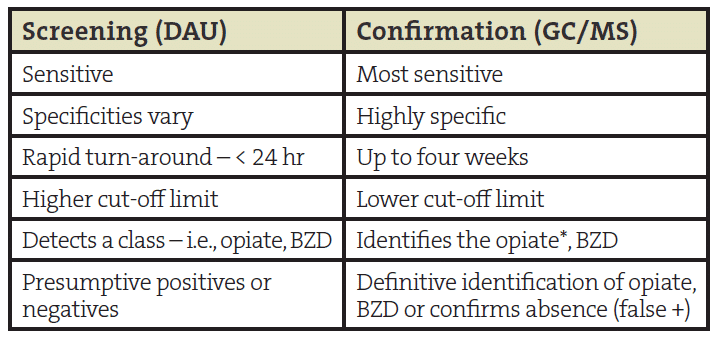
- Confirmation: GC/MS-confirms DAU result and identifies the drug.
- To order: Consult, lab consult, DAU confirmation outpt.
- False positives: To rule out (or in) especially amphetamine, BZD, other unexpected results.
Miscellaneous
Heroin: 6-MAM in ~6-8hr, then morphine
- Only the presence of 6-MAM confirms heroin:
- + THC with passive exposure highly ulikely;
- Poppyseed-+morphine, patient counseled to abstain; or next positive will be assumed to be illicit.
- Low dose or PRN use-may not be + on DAU or confirmation
- Consider pill counts mid-prescription for actual use:
- High dose oxycodone expect parent drug and metabolite i.e., oxycodone AND oxymorphone.
- Absence of oxycodone implies not taken recently, oxymorphone can last 1-2 days after oxycodone.
- Morphine can also confirm for hydromorphone.
- Vicodin-hydrocodone or hydrocodone and hydromorphone or hydromorphone alone.
Approach to Opioid Tapering in the Patient without Addiction: BETTa
- Identify all Biopsychosocial treatment targets.
- Educate patient about pain contributors and benefits of opioid tapering.
- Treat all targets using an evidence-based, collaborative approach.
- Taper opioids very slowly – <10% of total daily dose every 1-2 months for those on chronic treatment.